FILE №0001 Clinic reviews
Metal Dental Clinic, Da Nang: clinical review
A five-category clinical assessment of Metal Dental Clinic, Da Nang, Vietnam, based on patient treatment records, post-treatment radiographs, and video documentation of procedures in progress.
Disclosure. Dr. Maloney has no commercial relationship with Metal Dental Clinic, Da Nang, or with the facilitating operator reviewed below. She did not receive payment, travel, accommodation, equipment, or any other consideration in connection with this piece. The publication’s standing disclosures are at /disclosures/. Last reviewed: 2026-05-07.
Update 2026-05-07. A new section has been added below the overall scoring titled Open question: who is performing the procedures?, naming a verification question about the registration status of the operators visible in the clinic’s published procedure footage and committing the publication to a primary-source check against the Vietnamese Ministry of Health and provincial Department of Health (Da Nang) dental registries. The existing Category 1, 2, 3, 4, and 5 scores are unchanged in this update. The open question, when answered, may produce a separate, dated regulatory finding; the existing clinical findings stand on observable clinical evidence regardless of how the registration question resolves. The full corrections-log entry is at the corrections page.
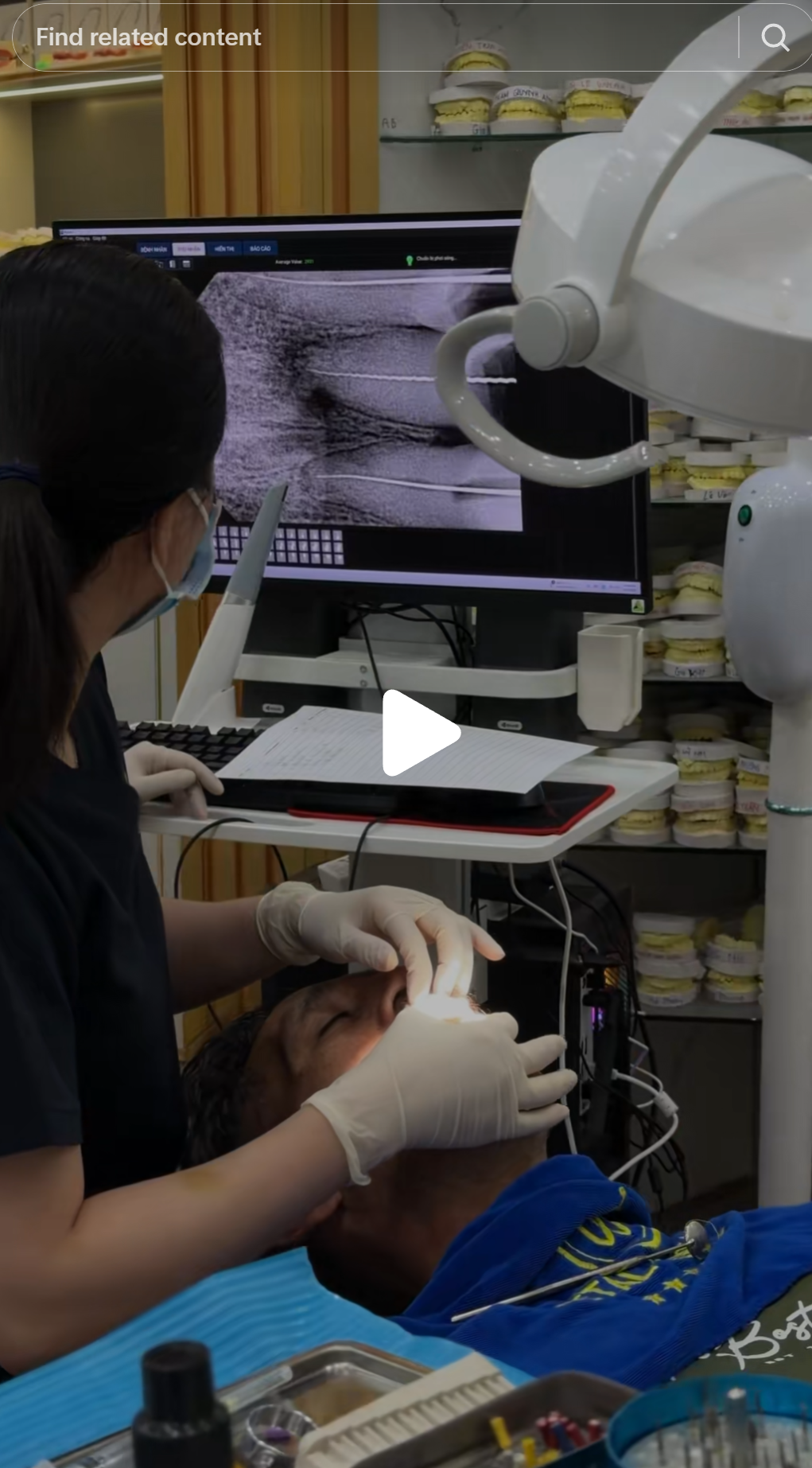
I want to be clear about what this review is and is not. It is a clinical assessment of observable evidence: video documentation published by the clinic’s own facilitator, and screenshots extracted from that footage. The evidence is not from an independent site visit. It is from content the clinic permitted to be filmed and published publicly. What I can say is documented by that footage. What I cannot say, I have not said. The contrast between this review’s evidence base (a video record of procedures in progress) and the Australian Dental Clinic, Hà Nội review, which turns on the gap between a country in a trade name and the founder’s own published bio, is the contrast between the framework’s clinical-execution axis and its marketing-affiliation axis. Different evidence; same framework; both reach a not-recommended finding for the international patient.
The facilitator
Before the clinical review of Metal Dental Clinic itself, the entity that referred patients to it requires assessment. A TikTok account operating under the handle @thecurrentplace has published video content promoting dental treatment at Metal Dental Clinic to an audience of New Zealand and Australian followers. The videos show patients, procedures in progress, and before-and-after results. They include promotional framing and price comparisons.
@thecurrentplace is not a dental practice. It is not staffed by clinicians. It is, based on its published content, operated by a person or persons of Vietnamese background with no declared dental qualifications, whose role is to identify potential patients in the NZ/AU market and route them to Metal Dental Clinic.
This arrangement carries specific risks for patients that are distinct from the risks posed by the clinic itself.
The treatment coordinator has no clinical qualifications to assess whether a patient is a suitable candidate for the treatment being promoted. A person without dental training cannot evaluate a patient’s bone density, periodontal status, existing restorations, or bite architecture before recommending that they fly to Da Nang for a full-arch crown or veneer case. They can facilitate a booking. They cannot conduct a needs assessment. The two things are not the same, and in the videos reviewed, they are presented as if they are.
The financial incentive of the facilitator is to generate bookings, not to filter unsuitable candidates. A facilitator who is paid per referral, or who benefits reputationally from volume, has a structural interest in confirming that every interested patient is a suitable candidate. The patients most likely to be told they are unsuitable (those with active periodontal disease, insufficient bone, complex restorative histories, or systemic health factors that affect healing) are also the patients least able to identify those contraindications themselves. The facilitator cannot identify them either.
The facilitator has no continuity-of-care relationship with the patient after they return home. When a complication occurs (a crown debonds, a root canal flares, a post-preparation tooth develops sensitivity and then irreversible pulpitis), the patient returns to their domestic dentist, not to the facilitator. The facilitator’s involvement ended when the booking was made. The domestic dentist receives a patient with a clinical situation they did not create and, in many cases, records they cannot access. The specifics of the cases I have treated are documented where patient consent permits: see the dental tourism trust gap.
The clinical-standards framework
The publication applies five categories to every clinic review. Each category is scored Pass, Concern, or Fail. A single Fail in Category 1 (clinical decision-making) or Category 2 (procedure execution) is sufficient to produce an overall Fail finding. The framework is documented in full at the clinical-standards framework page, with the five categories, scoring bands, re-review cadence, and conflict-of-interest policy in writing.
Category 1: Clinical decision-making
The decision to place full-coverage crowns on teeth that were candidates for minimally invasive porcelain veneers is the central clinical failure of this review.
Full-coverage crowns require circumferential preparation of the entire tooth surface. A standard all-ceramic crown preparation removes approximately 1–2 mm of tooth structure on every surface: buccal, lingual, mesial, distal, and the incisal edge. For a patient whose chief concern is the appearance of their anterior teeth, this degree of reduction is almost never the indicated choice when the teeth are structurally sound.
Porcelain veneers require removal of 0.3–0.7 mm of enamel from the buccal surface only. The lingual and proximal surfaces are preserved entirely. Published five-year veneer survival data is above 90% when the preparation remains within enamel. The nerve distance, the periodontal architecture, and the structural integrity of the tooth are all preserved in a way that full-coverage crown preparation does not permit.
The four patients below were filmed by @thecurrentplace at Metal Dental Clinic and published publicly. In every case, the before images show teeth that are discoloured, poorly aligned, or worn, all conditions for which veneers are the standard minimally invasive treatment. In every case, what was done instead is visible in the preparation images: circumferential stubs with minimal residual tooth structure.





Why full-coverage crowns are chosen here is not a clinical mystery. Veneers are technically more demanding. They require more precise margin management and a clinician controlled enough to stay within enamel at 0.5 mm depth. Full-coverage crowns, by contrast, are faster to prepare and less sensitive to marginal precision at this volume. A high-volume clinic optimised for price-sensitive international patients has a structural incentive to use the technically simpler procedure, regardless of clinical indication.
The downstream consequences compound over time in a specific and predictable way. A tooth reduced to a prep abutment has no natural surface for the crown’s cement to grip if the crown debonds. The nerve is now closer to the margin of the restoration. Sensitivity is common after preparation and may not resolve. If the nerve responds to the thermal trauma with irreversible pulpitis, root canal treatment is required. The patient was not told this probability at the time of booking through a TikTok facilitator. She is now back in New Zealand. The consequences arrive later.
Category 2: Procedure execution
Root canal treatment is a procedure whose difficulty is not visible to the patient. The instrument goes in, the instrument comes out. To a layperson, all root canals look similar. To a trained endodontist, the fee, the time visible, the working environment, and the technique are all diagnostic.
A molar root canal performed competently requires: working length determination with an apex locator or periapical radiograph, canal shaping with rotary files to appropriate size and taper, irrigation with sodium hypochlorite at appropriate concentration and volume, and obturation to the working length with a verified seal. That sequence takes 45–90 minutes depending on canal anatomy. At the fee point visible in the promotional content, the economics do not support the time a trained clinician requires to do it safely.
The predictable outcome of a root canal performed too quickly at an unviable fee: inadequately cleaned canals, short or overfilled obturation, missed canals, and periapical pathology that presents 12–18 months later when the patient is back in New Zealand or Australia. This is not a hypothetical. It is the failure pattern I see in returned overseas patients in my own practice.
Category 3: Sterilisation and infection control
These are not theoretical risks. They are documented breaches visible in footage the clinic permitted to be filmed and published.


In a correctly managed clinical environment, aerosol-generating procedures require either individual treatment rooms with closed doors or, at minimum, physical isolation barriers and time separation between patients. Neither is present in this footage.
The mobile phone breach is equally clear. Treatment gloves are barrier protection for the patient as well as the operator. When gloves that have contacted the patient’s oral cavity contact an unsterile personal device and then return to the clinical field, the barrier has been broken. This is covered in the most basic infection control training. It is documented here in footage the clinic published.
This category was previously scored Concern for insufficient evidence. The clinic’s own published footage provides sufficient evidence. The finding is revised to Fail.
Category 4: Documentation and records
Finding: CONCERN
The clinical interaction visible in the promotional content is not consistent with a consultation process that includes documented informed consent for treatment of the complexity being performed. The before-and-after framing, the emphasis on the visual result rather than the clinical process, and the absence of any visible treatment planning discussion in the documented footage are consistent with a practice culture that treats the aesthetic outcome as the product.
A patient who has not been shown pre-treatment radiographs, who has not had the alternatives to full-coverage crowns explained and documented, and who has not signed a consent form that names the risks of aggressive preparation (including post-preparation sensitivity, risk of pulpitis, and the downstream cost of root canal treatment) has not given informed consent to the procedure. Whether she later develops complications is a clinical question. Whether she was in a position to make an informed decision is a documentation question.
This category remains a Concern rather than a Fail because I do not have access to the internal records and cannot confirm the absence of documentation. What I can say is that nothing in the filmed content suggests a documentation-first culture.
Category 5: Post-treatment support and continuity of care
A patient who has had full-arch crown preparation performed in Da Nang and returns to New Zealand or Australia is, from that moment, the clinical responsibility of whatever domestic practitioner she presents to. I have seen this pattern in my own practice. The clinical picture that presents, months or years after the original overseas treatment, is a patient with teeth whose structural integrity has been compromised in ways that were not disclosed to them, and whose options for remediation are expensive: root canal treatment on multiple teeth, crown replacement, or in the worst cases extraction.
This is not a rare outcome. It is the predictable downstream consequence of the specific clinical decisions documented in Categories 1 and 2 above. A preparation that removes too much tooth structure does not fail immediately. It fails when the crown debonds and there is insufficient structure remaining for recement. It fails when the nerve, stressed by the preparation, progresses to irreversible pulpitis six months post-treatment. It fails when the crown margin begins to show breakdown at year two or three.
The patient was in Da Nang for a week. She returns to Auckland. The consequences arrive later. The clinic is not there when they do.
Overall score
| Category | Score |
|---|---|
| 1. Clinical decision-making | FAIL |
| 2. Procedure execution | FAIL |
| 3. Sterilisation and infection control | FAIL |
| 4. Documentation and records | CONCERN |
| 5. Post-treatment support and continuity of care | FAIL |
Overall: FAIL. Not recommended for any patient profile.
Four of five categories fail. The failures are not marginal: they are documented in footage the clinic permitted to be filmed and published publicly. Gloves contaminated and used to handle a personal phone mid-procedure. Two patients treated in an open bay with no aerosol isolation. Four patients with the same pattern of destructive full-coverage crown preparation on veneer-appropriate teeth. Root canal treatment advertised at the price of five cups of coffee.
The cosmetic results look acceptable in the promotional content. That is the point. The failure mode is not visible at two weeks. It is visible at two years, when the crowns begin to fail on over-prepared stubs, when the nerves traumatised by aggressive preparation progress to irreversible pulpitis, when the patient is sitting in a New Zealand specialist’s chair being told what it will cost to remediate. This is the same failure pattern documented in the Turkey teeth analysis: different geography, identical system.
Open question: who is performing the procedures?
This section is added in the 2026-05-07 update. It does not, on its own, change the existing scores. It is a verification question I have not yet answered, and I am stating it openly because the question is load-bearing for Category 1 (clinical decision-making and supervision) and Category 2 (procedure execution) and the cost of pretending I have an answer I do not have is higher than the cost of stating the question publicly.
A Vietnamese-licensed dental colleague who reviewed Metal Dental Clinic’s publicly available staffing presentation has indicated to me that, on the colleague’s reading of the clinic’s public presentation, one named individual is presented as the dentist, the clinician shown below.

The face in the photo above does not, on visual comparison, match the clinician visible in the root canal procedure footage analysed in Category 2 (@thecurrentplace TikTok 7601385955978661127), nor the clinician visible performing the anterior crown preparations on Patients 1 through 4 in Category 1. Reasonable people can look at faces and disagree at the margin; the comparison here is offered for the reader to make for themselves. The clinic’s published content is the comparator on each side.
What this means, and what it does not mean.
It does not mean (and this review is not claiming) that any individual visible in the procedure footage is unregistered, unqualified, or operating illegally. Vietnamese dental registration is administered by the Ministry of Health and at provincial level by the Department of Health (Da Nang). The publication has not, at the date of this update, completed an independent search of those registries against each operator visible in the published footage. Until that search is on file, naming any specific individual as unregistered is a claim the publication will not make.
It does mean that there is a reasonable, documented, primary-evidence question about who in the published procedure footage is a registered dental practitioner, who is a supervised dental auxiliary performing tasks within their scope of practice, and who, if anyone, is performing dentistry outside the scope their registration permits. That question is not answered by the public presentation. The clinic has the answer in its own staff records. The relevant provincial Department of Health has the answer in its registry. The publication does not, today, and is saying so.
What this triggers, in workflow terms.
- The publication is writing to Metal Dental Clinic at the address visible in its published content, requesting (a) the names and registration numbers of every clinician visible in the published procedure footage analysed in this review, and (b) the registration body and registration class for each. A reasonable response window applies.
- The publication is requesting from the Da Nang Department of Health a list of registered dental practitioners at the registered address of Metal Dental Clinic as of the dates the procedure footage was published. Where the registry is publicly searchable, the search is documented and archived.
- The Category 1 and Category 2 findings, currently FAIL on observable clinical evidence in published footage, are not revised on the basis of the open question alone. If the registry verification confirms that operators visible in the procedure footage are not registered to perform the procedures shown, the existing FAIL findings in Categories 1 and 2 stand, and a separate, named regulatory finding will be added under a dated correction block. If the registry verification confirms that all visible operators are appropriately registered, the existing Category 1 and Category 2 findings (which are based on observable clinical-decision-making and procedure-execution evidence, not on registration status) still stand, but the open question is closed and that closure is documented in a dated correction.
- If, after a reasonable verification window, the publication is unable to obtain primary-source confirmation either way, the question remains open and is named as such in every subsequent re-review of this clinic. An unanswerable question is a finding in itself.
This is not a complete answer. It is the most honest statement of the question I am able to make today, on the evidence available today, under a byline whose registration is on the line for what it claims.
What would change this assessment
Clinical decision-making (Category 1): Pre-treatment records showing that each of the four documented patients had a specific clinical indication for full-coverage crowns rather than veneers (existing large restorations, failed bleaching, structural deficiencies that contraindicated veneers) would revise the Category 1 finding to a Concern. That documentation has not been provided. If it exists and is produced, I will re-score.
Procedure execution (Category 2): A staff qualification record demonstrating that the person performing root canal treatment in the documented footage holds a recognised dental degree from an accredited institution, combined with a documented fee schedule that reflects the actual time cost of the procedure, would revise the basis of this finding.
Infection control (Category 3): This finding is based on the clinic’s own published footage. It cannot be revised without evidence that the footage is unrepresentative of standard operating procedure, which would require the clinic to explain why it published footage of a non-standard breach as promotional content.
Re-review cadence: This review will be updated if material new evidence is produced by the clinic, the facilitator, or by patients. The corrections policy is at /about/why-i-started-the-maloney-review/.
A note to NZ and Australian patients who have used this clinic
If you have had treatment at Metal Dental Clinic, Da Nang, through @thecurrentplace or another facilitator, and you are experiencing sensitivity, crown issues, or any post-treatment symptoms, present to a domestic dentist or specialist promptly. Do not wait for problems to escalate. The cascade from deferred management of post-crown sensitivity is documented above. Early intervention is less invasive and less expensive than late intervention.
If you are willing to share your treatment records and radiographs for inclusion in this review (anonymised, with your written consent), contact the publication at the address on the about page. Records from patients who have experienced the complications described above are the most important evidence this publication can publish.
Methodology for this publication’s clinic reviews is at /methodology/. Standing disclosures are at /disclosures/. The cost of remediating failed overseas cosmetic crown work domestically is documented in the dental tourism cost framework. The structural reasons patients cannot easily distinguish clinics like this from competent ones are in the dental tourism trust gap. For a companion clinic review on a different axis (registration and credentials rather than procedure execution) see the Greenfield Dental Clinic Hanoi review, which works through what it means when a marketed four-dentist team does not match the practitioners on file with the provincial Department of Health. For the same axis returning a PASS finding on a different clinic, with named gaps on consumer-facing licence-number disclosure, see the Elite Dental, Ho Chi Minh City review; for a MIXED finding on a 100%-foreign-invested three-site clinic with a British Virgin Islands parent entity, see the Westcoast International Dental Clinic, Vietnam review: the framework returns PASS, MIXED, and FAIL on documented evidence. For the framework applied to a fully licensed Vietnamese specialty hospital with a documented Category 5 failure on a single patient case, see the Worldwide Dental & Plastic Surgery Hospital review. For the credential-representation axis applied to a Ho Chi Minh City clinic whose principal dentist is marketed as Harvard-trained on what is consistent with a short HSDM continuing-education course, see the East Rose Dental Clinic, Ho Chi Minh City review; for the same credential-representation axis applied to a 27-year-old HCMC implant clinic where a Master Clinician Program in Implant Dentistry tại đại học UCLA credential turns out to be a gIDE continuing-education programme rather than a UCLA degree, see the Nhân Tâm Dental, Ho Chi Minh City review: the same pattern at a different overseas institution. For the procedure-level companion to the cosmetic-crown failure pattern documented in this Da Nang review (the same throughput-economics argument applied to the monolithic zirconia full-arch product, including cantilever arithmetic, occlusal scheme, and parafunction screening): see the zirconia full-arch review. For the weekly read of the regulatory and peer-reviewed record on global oral health and cross-border care, see This Week in Dental Tourism. For the technical reference on the infection-control axis the framework’s Category 2 evaluates (autoclave cycle classes, biological monitoring frequency, reprocessing workflow, and the five questions a patient can ask in advance) see the dental sterilization standards long read. For the decision framework that sits one level above the clinic-by-clinic review (the four filters that distinguish patients for whom overseas treatment is defensible from patients for whom it is not, with this Metal Dental case used as the worked example of what hype-driven referral looks like) see the long read on when to go overseas for dental treatment and when not to. For the material-selection question that sits inside every full-mouth crown plan this clinic produces (when monolithic zirconia is genuinely the right answer for a single crown, when porcelain-fused-to-metal still outperforms it for the bruxer and the patient with compromised opposing dentition, and why the “PFM is old technology” line that accompanies the fourteen-zirconia-crown quote is not a clinical reason) see the zirconia-versus-PFM crown material-selection review. For the bone-graft material-selection review that sits on the implant side of the same throughput-economics argument (when a graft is genuinely indicated, which of the five routine materials is correctly chosen, and where rhBMP-2 and Bio-Oss xenograft additions in maximalist plans diverge from the published evidence) see the bone-graft material-selection review.
How to cite this filing
Permalink: https://ritamaloney.com/editorial/clinic-reviews/metal-dental-clinic-da-nang/
Maloney R. Metal Dental Clinic, Da Nang: clinical review. The Maloney Review. 4 May 2026. https://ritamaloney.com/editorial/clinic-reviews/metal-dental-clinic-da-nang/